
Endometriosis is a common gynaecological condition, estimated to affect around 1 in 10 women of reproductive age in Singapore, and yet, many silently live with the pain, not realising how much it could be affecting their fertility too.
If you’ve been trying without success, your doctor may recommend assisted reproductive treatments such as Intrauterine Insemination (IUI) or In Vitro Fertilisation (IVF). Understanding the options available to you can help you feel more informed and prepared as you navigate your fertility journey.
What is endometriosis?
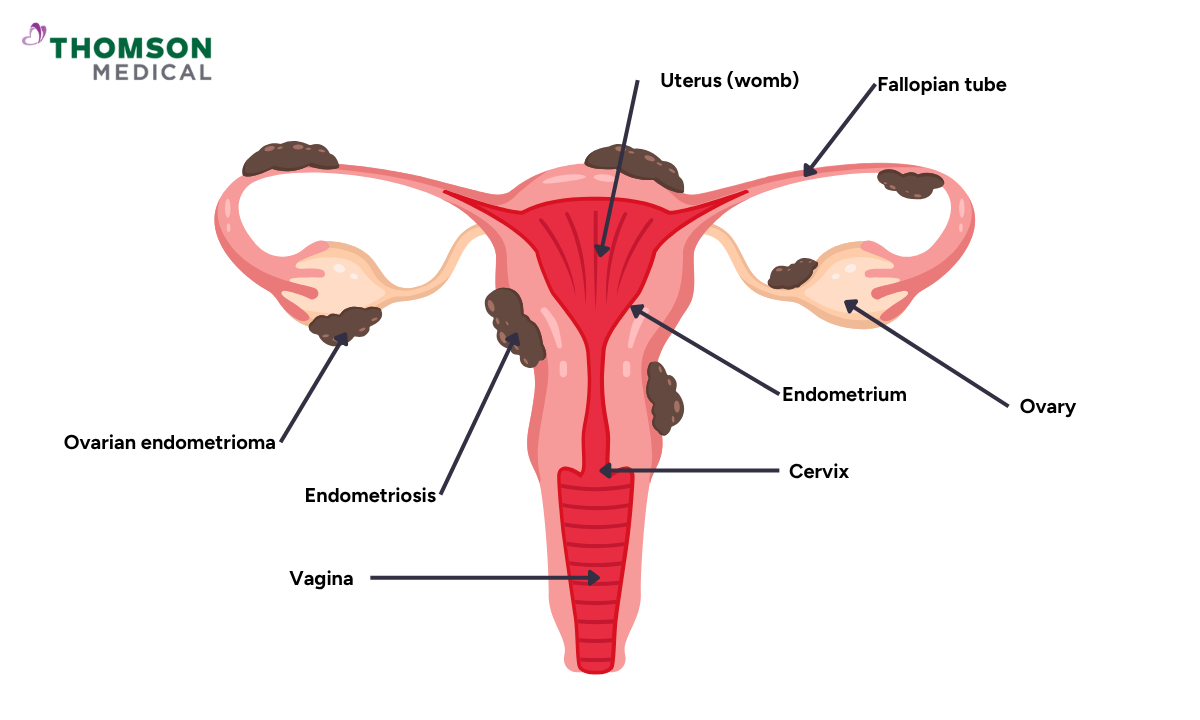
Endometriosis is a condition where tissue similar to the lining of your womb (endometrium) grows outside of its normal location. The endometrial-like tissue can grow in various locations throughout your pelvis, most commonly on your ovaries, fallopian tubes, and the tissue lining your pelvis.
In rare cases, it may also be found in more distant locations such as the intestines, bladder, or even the lungs. When it grows in the area it's not supposed to be, it may cause inflammation and scarring to the surrounding tissue in some cases.
This condition can affect women throughout their reproductive years, from adolescence onward, and is most commonly diagnosed in women in their 20s and 30s. However, endometriosis can also affect younger women during their teenage years.
How does endometriosis affect fertility?
Endometriosis can make it harder to get pregnant because it often grows on or around the reproductive organs. Here’s how it might affect your chances of conceiving:
Reduced ovarian reserve:
When endometrial tissue forms on your ovaries (called endometriomas), it may damage them and reduce the number of available eggs in them (ovarian reserve).
Tubal blockage:
If endometrial-like tissue grows around your fallopian tubes, it can cause blockages that prevent sperm from reaching the egg and fertilising it.
- Your doctor can detect it through hydrosalpinx ultrasound
Pelvic inflammation:
This condition can cause chronic inflammation that can affect reproductive organs, making the environment less conducive to implantation.
Egg quality:
Endometriosis may also negatively impact egg quality, reducing the chances of successful fertilisation and healthy embryo development.
Hormonal disruption:
Since endometriosis also affects ovulation, the time between ovulation and the next period (luteal phase), and the endometrial receptivity to fertilised eggs, this condition can also lead to hormonal disruption inside the body.
If you are experiencing symptoms or have concerns about how endometriosis may be affecting your fertility, speaking with a specialist can help you understand your options and which steps may be appropriate for you. For further assessment and tailored treatment options, schedule a consultation with Thomson Fertility Centre.
Stage of endometriosis
Based on the severity and location of the tissue growth, endometriosis can be classified into four stages:
Stage I (minimal):
During this early stage, there are small patches of endometrial tissue that grow outside of the womb with little to no scarring around the growth.
Stage II (mild):
If the condition progresses, there are more areas that are affected by the endometriosis growth. However, these implants are relatively small with no scarring or tissue damage.
Stage III (moderate):
During this stage, multiple deep implants of abnormal tissue are present, along with the formation of small cysts on one or both ovaries.
Adhesions (scar tissue that causes organs to stick together) or ovarian endometriomas may also be present around the fallopian tubes or ovaries.
Stage IV (severe):
At this most severe stage, there is extensive abnormal growth throughout the pelvic area, large ovarian endometriomas, and significant scarring or adhesions that may cause organs to stick together.
Fertility treatment options for endometriosis
To improve your chances of conceiving, your doctor will usually recommend assisted reproductive technology (ART), such as Intrauterine Insemination (IUI) or In Vitro Fertilisation (IVF). The table provides an overview of what each procedure generally involves. Your doctor will advise on which approach may be most appropriate based on your individual circumstances.
| IUI | IVF | |
|---|---|---|
| Procedure | Your partner's sperm sample is collected and "washed" to select sperm that are most likely to be suitable for fertilisation. After this sperm preparation step, your doctor will inject sperm into your womb to allow natural fertilisation to occur in your fallopian tubes during ovulation. | During the IVF process, your doctor will first extract a mature egg from your ovaries. After the egg retrieval procedure, eggs and sperm are placed together in an incubator to allow fertilisation. Alternatively, the doctor can perform intracytoplasmic sperm injection (ICSI), where a single sperm is injected directly into a mature egg. The fertilised egg (embryo) is then placed back inside your womb. |
Invasiveness | The procedure is minimally invasive because it only requires the insertion of a catheter into your womb during the insemination process. | More invasive, to perform the egg retrieval procedures, a thin needle guided by a transvaginal ultrasound is used. Additionally, just like IUI, a catheter is required to insert the embryo into the womb. |
Cost | IUI is generally less costly than IVF because it is a less complex procedure. As a guide, treatment may cost from around SGD 1,500 in public healthcare institutions, while fees at private fertility centres may start from around SGD 2,000–3,000, depending on the treatment plan, medications and investigations required. | IVF is generally more costly than IUI because it involves additional laboratory procedures and medications In Singapore, the cost of one IVF treatment cycle may be around SGD 15,000 or more before applicable subsidies. Eligible patients may be able to use MediSave and, where applicable, government co-funding to help offset part of these costs, subject to prevailing eligibility criteria. |
Fertility medication | It can be used to help the release of the egg from your ovaries (ovulation); this procedure is called superovulatory IUI (SO-IUI). | The stimulation of the ovary is required to increase the number of eggs the ovaries produce. |
IUI or IVF for endometriosis
Before deciding on the right fertility treatment for you, your doctors will assess several factors, such as:
Your age
Your plans for future pregnancies
The severity of the endometriosis and your symptoms
Based on this evaluation, they will typically recommend treatment as follows:
For stages 1 and 2:
If your doctor's assessment shows that your condition is minimal or mild, you have a healthy egg reserve, and you are under 35 years old, you may benefit from IUI treatment.
This less invasive approach may be considered appropriate when endometriosis is at an earlier stage and reproductive organs remain largely unaffected, as assessed by your doctor.
For stages 3 and 4:
If your condition has progressed to the moderate or severe stage, with blocked fallopian tubes or signs of a reduced egg reserve, and if you are over 35 years old, your doctor may recommend IVF due to these changes and related risks.
However, in cases of severe ovarian endometriomas or adhesions, your doctor may recommend laparoscopic surgery to remove the abnormal tissue growth before proceeding with IVF treatment to improve your chances of treatment success.
To discuss which procedure would be most suitable for your condition, schedule a consultation with Thomson Fertility Centre. Our fertility specialist can provide more information about IUI and IVF fertility treatment, including their benefits and any potential risks.
Success rates of IUI vs. IVF in different stages of endometriosis
The success rates for each fertility treatment may vary depending on the stage of endometriosis. The following is intended as a general overview only. Individual outcomes vary significantly, and your fertility specialist is best placed to advise on what may be realistic for your personal circumstances.
IUI success rates
As a general reference, some published studies have reported IUI success rates of around 5–10% per cycle for stages 1 and 2 endometriosis, with rates tending to be lower for stages 3 and 4. These figures vary across studies and do not predict individual outcomes, which depend on a range of personal health factors.
Due to these lower success rates, your doctor may recommend proceeding directly to IVF treatment.
IVF success rates
Research suggests that IVF success rates tend to be higher in younger women and those with milder stages of endometriosis. Some studies have reported figures of around 40–50% per cycle for women under 35 with stage 1 or 2, reducing to around 30–40% for stage 3 and 20–30% for stage 4.
Where endometriosis is more advanced, your doctor may recommend laparoscopic surgery beforehand to help create more favourable conditions for IVF. As with all fertility treatment, individual outcomes depend on a range of personal health factors and can vary considerably.
FAQ
What age is best to get pregnant with endometriosis?
If you have endometriosis, the best time to conceive is before 35, when fertility and egg quality tend to be higher. However, conception may still be possible at older ages with appropriate medical support, though outcomes vary between individuals and a specialist can help you understand what may be realistic for your circumstances.
Under 35 years:
You have the highest chance of success with both IUI and IVF, this is generally considered a favourable period for family planning when living with endometriosis.
Aged 35 to 40:
Although fertility naturally begins to decline, IVF may still be an appropriate and worthwhile option to explore with your specialist. Your fertility specialist may recommend moving to IVF sooner rather than trying IUI first.
Over 40 years:
Egg quality and quantity decrease significantly, affecting IVF success rates. With appropriate medical support, conception may still be possible, and your fertility specialist can help you understand what options may be suitable for you.
What factors affect successful conception with IUI or IVF for endometriosis?
If you have endometriosis, there are several factors that influence your chances of conceiving with fertility treatments, including:
Your age
Your ovarian reserve
The stage of your endometriosis
Embryo and implantation environment
Surgical history of endometriosis removal
Sperm quality, including count, motility, and overall health
Pre-treatment with medications for moderate to severe endometriosis
Is IVF better than IUI for endometriosis?
The most appropriate fertility treatment depends on your individual circumstances. IVF may be recommended by your fertility specialist in situations such as:
Moderate to severe endometriosis (stage III or IV)
Blocked fallopian tubes or endometriomas
Previous IUI cycles that have not resulted in pregnancy
For some individuals with mild endometriosis, IUI may also be considered, depending on their fertility assessment and individual treatment plan.
Which IVF protocol is best for endometriosis?
The most effective protocol depends on your age, ovarian reserve, and the severity of your condition. There are two main approaches that your doctor may recommend:
The long GnRH agonist protocol (ultralong protocol):
Before starting IVF, you take special hormone medication for two to six months. This medication temporarily "switches off" your body's natural hormone cycle.
This aims to reduce endometriosis activity and inflammation in the pelvis, which may help support the body in preparation for IVF treatment.
Antagonist protocols:
With this approach, you start IVF treatment straight away and take medication for a shorter time. These medicines help regulate your cycle and reduce the risk of eggs being released too early.
This protocol is quicker and involves fewer injections and less waiting compared to the ultralong protocol.
How successful is IVF with endometriosis?
Research suggests that IVF may be a viable option for women with endometriosis, with outcomes influenced by factors such as age, stage of the condition and egg quality. Some published studies have reported the following figures as general reference points:
Stages 1 and 2 (minimal to mild): around 40–50% per cycle
Stage 3 (moderate): around 30–40% per cycle
Stage 4 (severe): around 20–30% per cycle, which may be supported by surgical treatment prior to IVF in some cases
These figures vary across studies and do not predict individual outcomes. Your fertility specialist will be best placed to discuss what may be realistic for your personal circumstances.
Can IUI be performed in cases of endometriosis?
Yes, intrauterine insemination (IUI) may be an option if you have mild to moderate endometriosis. It may increase your chances of becoming pregnant by placing prepared sperm directly into your womb at the time of ovulation. IUI may be suitable if:
At least one of your fallopian tubes is open to allow the sperm and egg to meet
Your partner's sperm has a good count and motility
You are ovulating regularly so that the doctor can determine the best time to perform the procedure
Your fertility specialist will perform a series of tests, such as endometriosis ultrasound scans and hormone blood tests, to check these factors and determine whether IUI is appropriate for you.
What is the success rate of IUI for endometriosis?
Based on published data, IUI success rates in the context of endometriosis tend to be modest overall, with some studies reporting figures of around 5–10% per cycle for stages 1 and 2, and lower rates for more advanced stages.
Individual outcomes vary depending on age, ovarian reserve and other personal health factors, and your doctor will advise on whether IUI is the most appropriate option for you.
If you're considering IUI or IVF as fertility treatments for endometriosis, schedule an appointment with Thomson Fertility Centre. Our fertility specialist will be able to provide you with personalised treatment and advice based on the stage of your endometriosis.
For more information, contact us:
Thomson Fertility Centre
- Paragon: 6252 7766
- Novena: 6399 3758, 8811 0358 (WA)