
When a doctor mentions a pedunculated fibroid, the name alone can feel alarming – but these stalked growths are almost always benign and far more common among women than you might realise. Understanding what they are, and what they are not, can take much of the worry out of your next specialist visit.
What is a pedunculated fibroid?
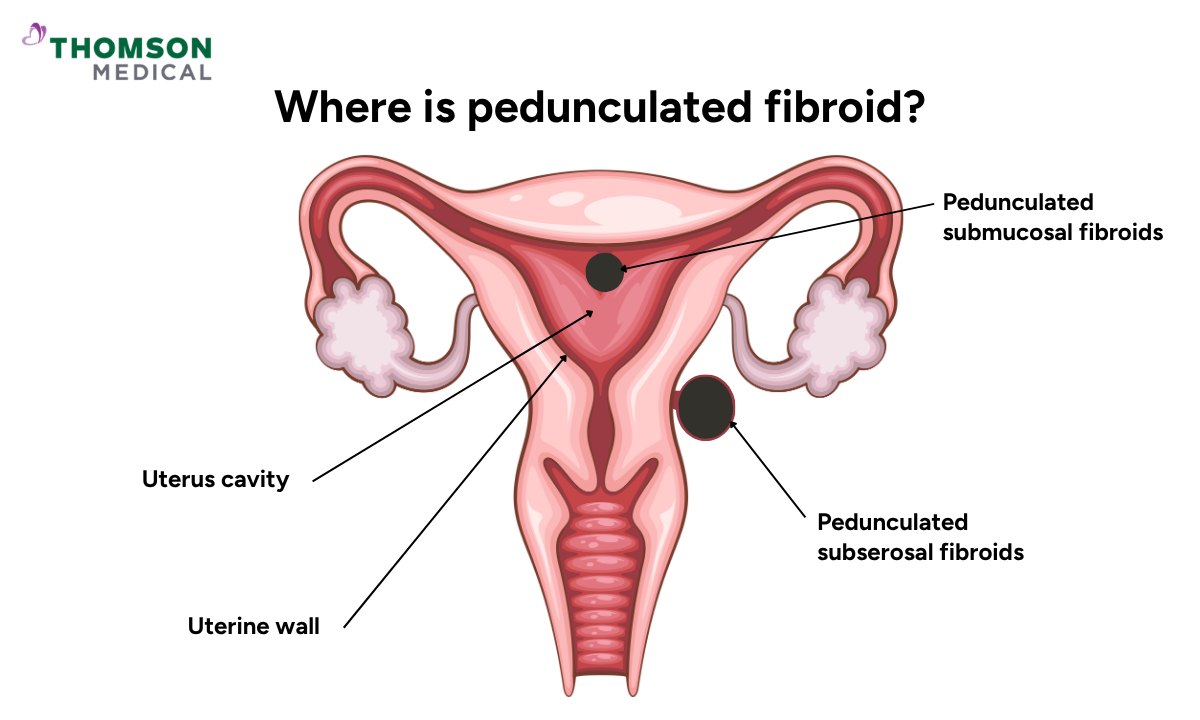
Uterine fibroids are benign (not cancerous) growths made of muscle and fibrous tissue that develop in or on the uterus. Most fibroids attach broadly to the uterine wall, but a pedunculated fibroid grows on a thin stalk that extends outwards from it. The term "pedunculated" simply refers to this stalk attachment.
There are two main types:
Pedunculated subserosal fibroids, which grow on the outer surface of the uterus and extend into the pelvic cavity
Pedunculated submucosal fibroids, which grow inwards into the uterine cavity
Because these fibroids are held in place by a narrow stalk rather than a wide base, they can shift position slightly within the pelvis.
What causes pedunculated fibroids?
Pedunculated fibroids develop for the same reasons as other uterine fibroids.
Factors linked to fibroid development include:
Hormonal changes involving oestrogen and progesterone
A family history of fibroids
Being in your reproductive years, particularly your 30s and 40s
Higher body weight, which may be linked to higher oestrogen levels
Fibroids may also become less active or shrink after menopause, when oestrogen and progesterone levels fall.
The fibroid stalk usually forms gradually as the fibroid grows, and its point of attachment to the uterine wall may become narrower over time. Most factors linked to fibroid development are not within your control, and developing one is never your fault.
What pedunculated fibroid symptoms might you notice?
Not every woman with a pedunculated fibroid experiences symptoms. In fact, some women only find out they have one during a routine scan.
When symptoms do occur, they may include:
Pelvic pressure or a feeling of fullness
Abdominal bloating or swelling
Heavy menstrual bleeding, particularly with pedunculated submucosal fibroids that grow into the uterine cavity
Frequent urination if the fibroid presses on the bladder
Constipation if the fibroid presses on the rectum
Pain can sometimes feel different with a pedunculated fibroid. Because the fibroid is attached by a stalk, there is a small chance the stalk can twist. This is called fibroid torsion, and it can cut off the fibroid's blood supply, leading to sudden, sharp pelvic pain.
If you develop sudden or severe pain in your pelvis or abdomen, please seek medical attention promptly, as this may need urgent assessment.
Our gynaecologists
Loading...
How are pedunculated fibroids diagnosed?
If you see your doctor with concerns about fibroids, the first step is usually a pelvic examination to check the size and shape of your uterus.
If fibroids are suspected, an ultrasound scan is often the next step. This uses sound waves to confirm whether fibroids are present, where they are located, and whether they are attached by a stalk.
In some cases, your doctor may also recommend an MRI scan for a more detailed view of the size, position, and number of fibroids. An MRI can be particularly helpful for pedunculated fibroids because it shows the stalk clearly, which supports treatment planning.
Pedunculated fibroids and pregnancy
Many women with pedunculated fibroids go on to have healthy pregnancies, so having one does not necessarily mean you will experience complications.
However, the size and location of the fibroid can influence how it may affect your pregnancy:
Pedunculated subserosal fibroids, which grow on the outer surface of the uterus, are less likely to interfere directly with pregnancy
Pedunculated submucosal fibroids, which grow into the uterine cavity, may raise the risk of miscarriage or other complications during pregnancy
Larger fibroids may become more uncomfortable as your uterus expands during pregnancy
In some cases, hormonal changes and increased blood flow during pregnancy can lead to fibroid pain or a process called degeneration, where the fibroid outgrows its blood supply and starts to break down. This usually settles with rest and pain relief, but your doctor can guide you on what is right for your situation.
Many women with pedunculated fibroids go on to have healthy pregnancies, but regular follow-up can help identify any changes early. Request an appointment at Thomson Medical to get guidance on appropriate imaging, symptom monitoring, and pregnancy care tailored to your situation.
What are the treatment options for pedunculated fibroids?
When treatment is needed, the right approach depends on the size and location of the fibroid, the severity of your symptoms, and whether preserving fertility is important to you.
Medicines
Medicines cannot remove fibroids, but they may help manage symptoms while you consider further treatment or prepare for a procedure.
These may include:
Pain relief:
Over-the-counter medicines such as ibuprofen can help ease pelvic discomfort.
Hormonal therapy:
The contraceptive pill, hormonal injections, or an intrauterine device (IUD) may help regulate hormones and improve symptoms such as heavy bleeding.
GnRH medicines:
These medicines temporarily lower oestrogen and progesterone levels and may help shrink fibroids, particularly before surgery. They are generally used under close medical supervision and are not suitable for long-term use.
Medicines may help with pain or bleeding symptoms, but they do not remove the fibroid or correct torsion if the stalk twists. Symptoms may also return once treatment stops, which is why medicines are often used as a short-term measure alongside other treatments.
Minimally invasive procedures
If medicines are not providing enough relief, minimally invasive procedures may help treat the fibroid without major surgery.
These include:
Uterine artery embolisation (UAE):
Tiny particles are injected into the blood vessels supplying the fibroid, reducing its blood supply and causing it to shrink over time.
For pedunculated fibroids, your doctor will need to assess whether UAE is suitable, as the way the fibroid is attached by a stalk can affect how it responds to treatment.
If you are planning a future pregnancy, your doctor will discuss whether UAE, myomectomy, monitoring, or another approach is more suitable.
Laparoscopic myomectomy:
This procedure is performed through small incisions in the abdomen using a camera and fine instruments to remove fibroids while preserving the uterus.
The size, position, and stalk of your fibroid will influence which procedure is most appropriate. Your doctor will advise on which options suit your situation.
Surgical options
Surgery may be considered if symptoms are severe, complications develop, or other treatments have not been effective. Because pedunculated fibroids are attached by a stalk rather than deeply embedded within the uterine wall, they can often be removed more straightforwardly than other fibroid types.
Options include:
Myomectomy:
This removes the fibroid while preserving the uterus. This is frequently preferred when fertility preservation is important.
Hysterectomy:
This involves removing the uterus entirely and is usually considered when symptoms are severe, fibroids continue to recur, or a future pregnancy is not planned.
Hysterectomy is the only treatment that prevents fibroids from returning. With all other options, there is a chance that new fibroids may develop over time, which your doctor will discuss with you.
When to see a doctor
Pedunculated fibroids can sometimes cause symptoms or complications that are easier to manage when identified early.
It is worth speaking with your doctor if you notice:
Sudden pelvic pain, especially if it feels sharp or focused in one spot
A feeling of pressure or heaviness in one area of your pelvis
Bloating or a noticeable lump in your abdomen
Frequent urination or constipation
Heavy bleeding, particularly with pedunculated submucosal fibroids growing into the uterine cavity
Difficulty becoming pregnant or new fertility concerns
If you develop sudden, severe pelvic or abdominal pain, especially alongside nausea, vomiting, or fever, please seek urgent medical attention straight away. These can sometimes be signs of torsion, which needs immediate care.
Sudden severe pelvic pain should always be assessed promptly, particularly if a pedunculated fibroid may have twisted on its stalk. Request an appointment with Thomson Medical for timely evaluation and support tailored to your symptoms and reproductive goals.
FAQ
Do pedunculated fibroids need to be removed?
Not always. Removal is usually recommended only if pedunculated fibroids cause symptoms such as pain, heavy bleeding, fertility problems, rapid growth, or twisting of the stalk (torsion).
Do pedunculated fibroids cause pain?
Yes, they can. Pain is more likely if the fibroid is large and presses on nearby organs or if the stalk twists and cuts off the blood supply.
Can a pedunculated fibroid burst?
Pedunculated fibroids do not typically "burst". However, the fibroid can sometimes break down if it loses part of its blood supply. This is called degeneration, and it may cause pain. In some cases, degeneration may also be associated with fever, nausea, or discharge, depending on the type and location of the fibroid.
Can a pedunculated fibroid cause miscarriage?
Submucosal pedunculated fibroids that extend into and change the shape of the uterine cavity may increase the risk of miscarriage. Subserosal pedunculated fibroids, which grow on the outer surface of the uterus, are less likely to affect pregnancy.
What can cause a pedunculated fibroid to twist?
Twisting (also known as torsion) can happen when a fibroid attached by a long or narrow stalk rotates on itself. This may be more likely with a mobile pedunculated fibroid, during changes in uterine size, or during pregnancy, but it can also happen without a clear trigger.
Are pedunculated fibroids difficult to remove?
Pedunculated fibroids are often more straightforward to remove than fibroids deeply embedded within the uterine wall, because they are attached by a stalk. However, the complexity of surgical treatment still depends on factors such as the size, position, and blood supply of the fibroid.
The information provided is intended for general guidance only and should not be considered medical advice. For personalised recommendations and tailored advice based on your unique situations, please consult a specialist at Thomson Medical. Request an appointment with Thomson Medical today.
For more information, contact us:
Thomson Specialists (Women's Health)
Thomson Women's Clinic (TWC)
- Novena:
6592 6686 (Call), 8611 8986 (WA) - Bukit Batok:
6569 0668 (Call), 8686 3525 (WA) - Choa Chu Kang:
6893 1227 (Call), 8282 1796 (WA) Jurong:
6262 8588 (Call), 6262 8588 (WA)- Katong (female doctor):
6970 2272 (Call), 8611 9020 (WA) - Punggol:
6243 6843 (Call), 8811 0328 (WA) - Sembawang: 6753 5228
- Sengkang: 6388 8125
- Serangoon (female doctor): 6382 3313
- Tampines: 6857 6266
- Tiong Bahru: 6276 1525