
Heavy periods and pelvic discomfort are easy to write off as a normal part of life, but they are often the body's way of flagging something deeper. For many women, that something is intramural fibroids, growths that can quietly develop within the uterine wall without ever announcing themselves.
Knowing what intramural fibroids are, the symptoms they can cause, and the options available if treatment is needed can help you feel prepared and informed when you speak with your doctor.
What are intramural uterine fibroids?
Fibroids are benign (non-cancerous) growths that can develop in or around the uterus.
Intramural fibroids specifically grow within the muscular wall of the uterus, a layer known as the myometrium.
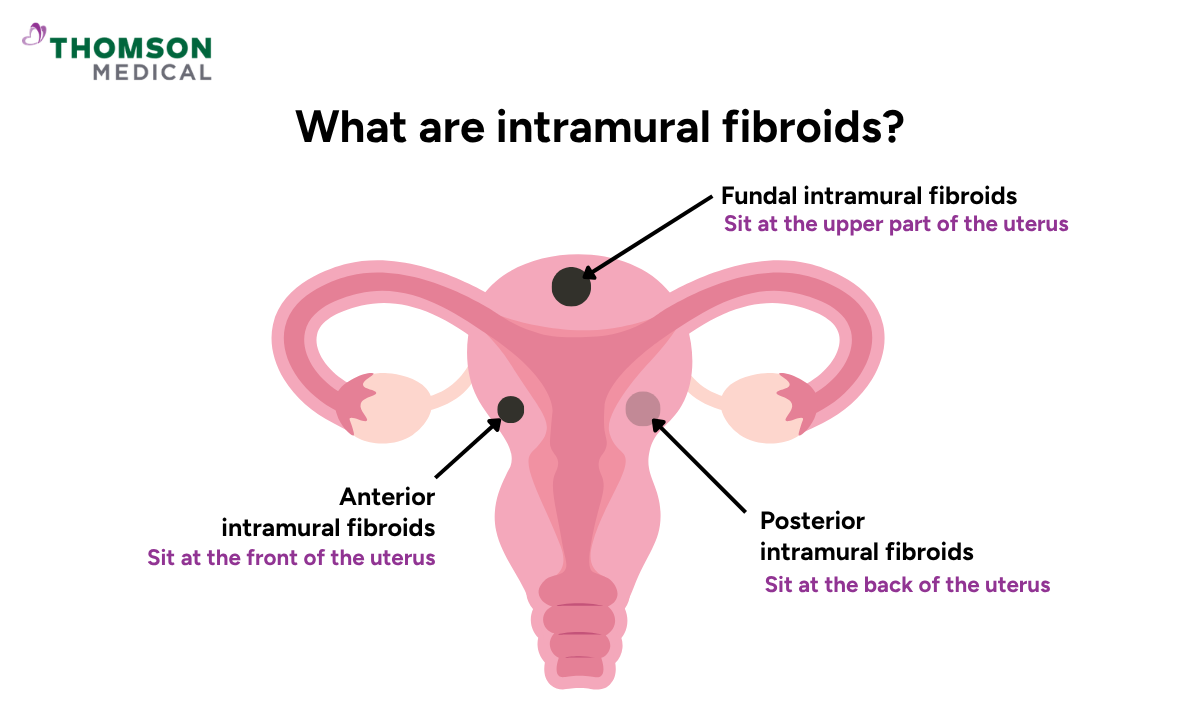
Intramural fibroids can also be described by where they sit within the uterus:
Anterior intramural fibroids sit at the front of your uterus
Posterior intramural fibroids sit at the back of your uterus
Fundal intramural fibroids sit at the upper part of your uterus
Position also shapes which treatment options are practical. Deeply embedded intramural fibroids can be harder to remove without affecting the surrounding uterine muscle, which influences both surgical planning and recovery.
What causes intramural fibroids?
Intramural fibroids begin when muscle cells in the uterine wall start to grow abnormally. Exactly why this happens is not fully understood, but the hormones oestrogen and progesterone appear to play a key role.
Because of this hormonal link, fibroids can behave differently at different stages of life:
They may grow during pregnancy, when higher oestrogen and progesterone levels, increased uterine blood flow, and pregnancy-related growth factors can create conditions that encourage fibroid growth
They often shrink after the menopause, when oestrogen and progesterone levels naturally fall
The rapid hormonal shifts and increased blood supply during pregnancy can speed up fibroid growth, which is why women with known fibroids are usually monitored more closely throughout.
What are the intramural fibroid symptoms?
Many women with intramural fibroids experience no symptoms at all. When symptoms do appear, they are usually similar to those of other fibroid types.
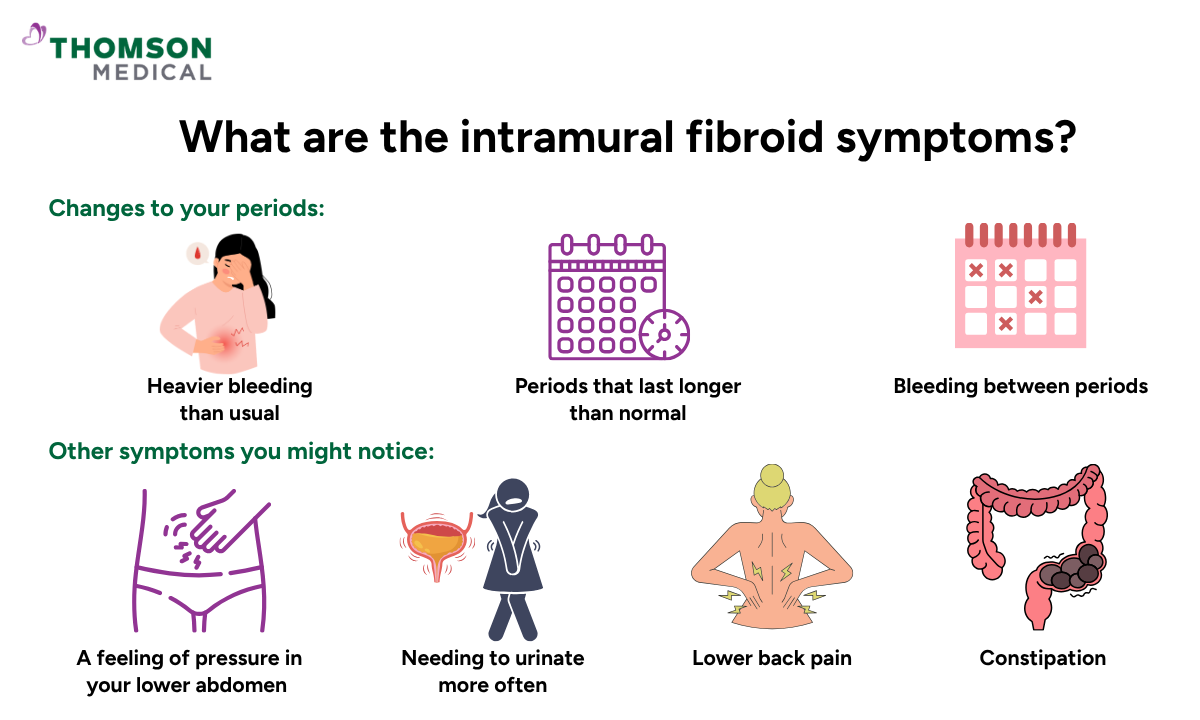
Changes to your periods:
Heavier bleeding than usual
Periods that last longer than normal
Other symptoms you might notice:
A feeling of fullness or pressure in your lower abdomen
Needing to urinate more often
Lower back pain
Constipation
These symptoms can vary from one woman to the next. Some find them mild and manageable, while for others they affect daily life more noticeably. If that sounds like you, it is a good idea to speak with your doctor soon.
Our gynaecologists
Loading...
How are intramural fibroids diagnosed?
If you visit your doctor with concerns about fibroids, they will usually begin with a pelvic examination to check for any changes in the size or shape of your uterus.
If fibroids are suspected, the next step is often an ultrasound scan. This is a straightforward, non-invasive test that can identify whether fibroids are present. In some cases, your doctor may also recommend an MRI scan, which provides a more detailed view of the size, number, and exact position of the fibroids.
In certain situations, additional procedures may be recommended, including:
Sonohysterography, a specialised ultrasound that uses fluid inside the uterus to create a clearer view of the uterine cavity
Hysteroscopy, a procedure where a thin camera is passed through the cervix to examine the inside of the uterus directly
These tests can help distinguish intramural fibroids from fibroids affecting the inner lining of the uterus.
Intramural fibroids can behave differently depending on where they sit within the uterine wall and how large they become. Request an appointment with Thomson Medical for a thorough assessment, including imaging and personalised guidance on suitable next steps for care.
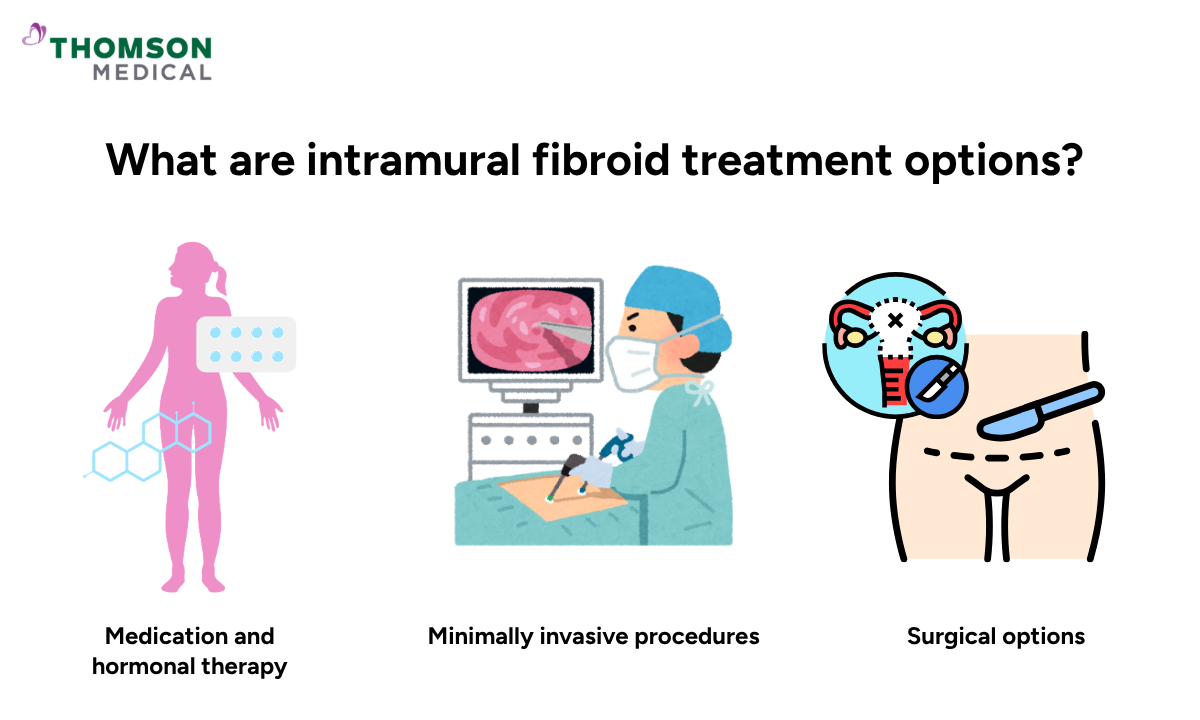
What are intramural fibroid treatment options?
Treatment is not the same for every woman. Your doctor will consider your symptoms, the size and location of your fibroids, your age, and whether you are planning a pregnancy before recommending the right approach for you.
Medication and hormonal therapy
If your symptoms are mild, medication is usually the first option your doctor will consider.
These include:
Pain relief:
Common painkillers such as ibuprofen may help ease discomfort during your period.
Iron supplements:
These can help replace iron lost through heavy or prolonged bleeding.
Hormonal therapy:
The contraceptive pill, injections, or an intrauterine device (IUD) can help regulate your hormones and reduce bleeding over time.
Tranexamic acid:
This non-hormonal medicine can help reduce heavy menstrual bleeding during your period.
GnRH agonists:
GnRH agonists temporarily lower oestrogen levels and may help shrink fibroids.
They are usually used for a limited period, sometimes before surgery, because longer use may cause menopause-like side effects.
Hormonal treatments help manage symptoms but do not remove fibroids. Once treatment stops, symptoms often return. For this reason, medication is usually used as a temporary measure, alongside or in preparation for another procedure.
Minimally invasive procedures
If medication alone is not enough, there are procedures that can treat fibroids without the need for major surgery.
Uterine artery embolisation (UAE):
Tiny particles are injected into the blood vessels that supply your fibroids, cutting off their blood supply and causing them to shrink.
Laparoscopic myomectomy:
Fibroids are removed through small incisions in the abdomen using a camera and fine instruments, with a shorter recovery time than open surgery.
Endometrial ablation:
The lining of the uterus is treated using heat, cold, microwave energy, or electrical current to reduce or stop heavy bleeding. It treats symptoms rather than fibroids themselves, as it does not remove or shrink the fibroids.
It is generally not recommended if you are planning a future pregnancy, so your doctor will discuss this carefully before recommending it.
Surgical options
For fibroids that are large, numerous, or deeply positioned, surgery may be the most appropriate route.
Surgical options include:
Myomectomy:
Removes fibroids through an incision in your abdomen. This is often recommended when there are multiple or very large fibroids, or when they are deeply embedded in the uterine wall.
Hysterectomy:
Removes the uterus entirely. This is usually considered when other treatments have not provided enough relief and a future pregnancy is not planned.
The choice between myomectomy and hysterectomy depends largely on whether preserving your uterus for a future pregnancy is important to you. For women who have completed their families, hysterectomy can be a lasting solution, as fibroids cannot return once the uterus has been removed.
Intramural fibroids and pregnancy
If you have been diagnosed with intramural fibroids and are thinking about starting a family, you may have questions about how they could affect your plans.
Here is what the evidence currently suggests:
Intramural fibroids do not usually prevent pregnancy from occurring
Fibroids may grow during pregnancy due to rising oestrogen levels, especially earlier in pregnancy. This can sometimes lead to discomfort or a feeling of pressure
Many fibroids shrink within six months of giving birth, as hormone levels return to normal
There may be a potentially increased risk of breech position, though many women with fibroids go on to have straightforward pregnancies
While fibroids do not usually affect pregnancy chances, it should be noted that larger fibroids, multiple fibroids, or fibroids that distort the uterine cavity may affect your fertility or pregnancy outcomes.
If you are pregnant or planning to conceive, let your doctor know about your fibroids early on. With the right monitoring and support, many women with intramural fibroids have healthy pregnancies.
When should you see a doctor?
Many women with intramural fibroids do not need immediate treatment, but certain symptoms are worth discussing with your doctor soon.
Speak to your doctor if you notice:
Periods that are becoming heavier, longer, or more painful over time
Pelvic pressure, cramping, or discomfort that does not improve
Frequent urination or constipation caused by pressure on nearby organs
Difficulty becoming pregnant or recurrent miscarriages
A feeling of fullness or enlargement in the lower abdomen
Any new bleeding after the menopause
For most women, intramural fibroids are manageable. Where treatment is needed, there are several options available, and your doctor can help you find an approach that suits your symptoms and your plans for the future.
Even when symptoms develop gradually, it is worth getting checked if something no longer feels normal for you. Request an appointment with Thomson Medical to evaluate your fibroid size, location, and whether monitoring or treatment may be appropriate.
FAQ
Is an intramural fibroid serious?
Intramural fibroids are generally not dangerous and are almost always benign. However, depending on their size and location, they can cause symptoms such as heavy bleeding, pelvic pain, or pressure on nearby organs that may require treatment.
Can intramural fibroids turn cancerous?
Intramural fibroids are benign growths that very rarely become cancerous. The risk of a malignant tumour such as uterine leiomyosarcoma is extremely low, occurring in fewer than 1 in 1,000 cases.
Can I get pregnant with intramural fibroids?
Yes, many women with intramural fibroids can conceive naturally and have healthy pregnancies. Although some fibroids may affect fertility depending on their size or location, most women go on to have healthy pregnancies.
Do intramural fibroids cause pain?
Yes, intramural fibroids can cause pelvic pain, cramping, or a feeling of pressure, especially as they grow within the muscular wall of the uterus. Symptom severity varies from woman to woman.
Is it necessary to remove intramural fibroids?
Removal is not always necessary. If intramural fibroids are small and do not cause symptoms, infertility, or complications, regular monitoring may be enough. Treatment is usually considered when symptoms affect quality of life or reproductive health.
Can intramural fibroids go away on their own?
Intramural fibroids usually do not disappear on their own during the reproductive years. However, they often shrink or become less symptomatic after menopause due to lower oestrogen and progesterone levels.
The information provided is intended for general guidance only and should not be considered medical advice. For personalised recommendations and tailored advice based on your unique situations, please consult a specialist at Thomson Medical. Request an appointment with Thomson Medical today.
References:
Coyle Institute. (2022, November 9). A closer look at the risk of cancerous fibroids. https://coyleinstitute.com/cancerous-fibroids/
For more information, contact us:
Thomson Specialists (Women's Health)
Thomson Women's Clinic (TWC)
- Novena:
6592 6686 (Call), 8611 8986 (WA) - Bukit Batok:
6569 0668 (Call), 8686 3525 (WA) - Choa Chu Kang:
6893 1227 (Call), 8282 1796 (WA) Jurong:
6262 8588 (Call), 6262 8588 (WA)- Katong (female doctor):
6970 2272 (Call), 8611 9020 (WA) - Punggol:
6243 6843 (Call), 8811 0328 (WA) - Sembawang: 6753 5228
- Sengkang: 6388 8125
- Serangoon (female doctor): 6382 3313
- Tampines: 6857 6266
- Tiong Bahru: 6276 1525